
- Development is related to age and presence of androgenic hormones/receptors
- Alopecia areata: Although exact etiology is unknown, there is a genetic predisposition, and consensus favors an autoimmune response
- Telogen effluvium: Normal hair cycle is interrupted so that anagen (growing) hairs are abruptly converted into telogen (resting) hairs, which are subsequently shed after 2 to 4 months
- Hypothyroidism and hyperthyroidism
- Postpartum, post-illness
- Surgery with general anesthesia
- Nutritional deficiency, particularly with iron or zinc
- Psychological stress
- Most telogen effluvium from medications is caused by retinoids, β-blockers, calcium channel blockers, antidepressants, and nonsteroidal anti-inflammatory drugs (including ibuprofen)
- Tinea capitis: Ringworm of the scalp in which dermatophyte fungus invades the hair shaft. The most likely dermatophytes include
- Microsporum (from cats and dogs)
SCARRING ALOPECIA
Also known as cicatricial alopecia, is hair loss that can ocure as a result of complications from another condition. In this type of alopecia the hair follicle is completely destroyed. Conditions that can cause scarring alopecia are:
- Growth disorders and inherited diseases (epidermal nevi-darier disease)etc
- Damages from natural causes ( mechanical trauma-burns ) etc
- Infections microbial or viral
- Neoplasia
- Various other skin diseases of unknown etiology.

NON -SCARRING ALOPECIA
CLASSIFICATION
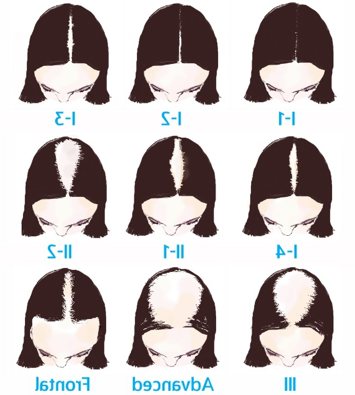
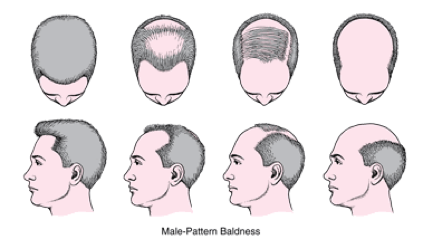
ANDROGENIC ALOPECIA
Genetically determined ( reason:Inheritance ) 95%for men and 75% for women
RISK FACTORS
- Family history of baldness
- Advanced age
- Physical stress
- Psychological stress
- Pregnancy
- Regular use of aggressive hair-styling techniques
- Poor nutrition
- Rapid weight loss
- Restrictive diets (eg, low carbohydrate, low fat)
EPIDEMIOLOGY
Incidence and prevalence:
- About 25% of men aged 25 years have some degree of clinically apparent androgenic alopecia
- About 42% of men develop androgenic alopecia
- About 2% to 3% of the general population develops alopecia areata